



{kind=link}
-
The Future Of Nano Technology

Categories
- Ai
- Alan Watts
- Anatomy
- Andropause
- Anti-Aging Medicine
- Arthritis
- Artificial General Intelligence
- Artificial Intelligence
- Artificial Super Intelligence
- Ataxia
- Autism
- Biochemistry
- BioEngineering
- Biotechnology
- Bitcoin
- Chemistry
- Cryonics
- Cryptocurrency
- David Sinclair
- Dementia
- Diet Science
- Diseases
- Eczema
- Elon Musk
- Futurism
- Gene Medicine
- Gene Therapy
- Gene therapy
- Genetic Medicine
- Genetic Therapy
- Global News Feed
- Healthy Lifestyle
- Healthy Living
- HGH Physicians
- Hormone Optimization
- Hormone Replacement Therapy
- Hormone Replacement Treatment
- Human Genetic Engineering
- Human Immortality
- Human Longevity
- Human Reproduction
- Hypogonadism
- Hypopituitarism
- Hypothyroidism
- Immortality
- Immortality Medicine
- Inflammation
- Injectable Growth Hormone
- Integrative Medicine
- Life Skills
- Longevity
- Longevity Medicine
- Low T
- Machine Learning
- Mars Colony
- Medical School
- Menopause
- multiple-sclerosis
- Nano Medicine
- Nanomedicine
- Nanotechnology
- Neurology
- Parkinson's disease
- Pharmacogenomics
- Protein Folding
- Psoriasis
- Quantum Computing
- Regenerative Medicine
- Resveratrol
- Sermorelin Physicians
- Singularity
- Spacex
- Stem Cell Therapy
- Stem Cells
- Stemcell Therapy
- Testosterone
- Testosterone Physicians
- Transhuman
- Transhumanism
- Transhumanist
- Uncategorized
- Veganism
- Vegetarianism
- Vitamin Research
- Wellness
-
Recent Posts
- Cheap longevity drug? Researchers aim to test if metformin can slow down aging : Shots – Health News – NPR
- The U.S. Needs to ‘Get It Right’ on AI – TIME
- Big Tech keeps spending billions on AI. There’s no end in sight. – The Washington Post
- Racist AI Deepfake of Baltimore Principal Leads to Arrest – The New York Times
- A Baltimore-area teacher is accused of using AI to make his boss appear racist – NPR
Archives
Popular Key Word Searches
- centraltph
- bicarbonate and growth immunity ray peat
- vrcc neurology
- bibliotecapleyades/amrita-longevity-immortality
- cbr xmen anatomy
- Medical genetics wikipedia
- immortality medicine
- GrabPay
- Grab Pay Philippines
- GrabPay Vietnam
- GrabPay Philippines
- dr weil psoriasis
- what does recovered mean covid-19
- tony pantalleresco
- tony pantalleresco herbalist book
- herbsplusbeadworks
- herbsplusbeadworks website
- hailie vanderven
- princeton longevity center scam
- aetna genetic testing policy
- anatomy of hell
- biggie
- longevity claims
- augmentinforce tony pantalleresco
- tony pantalleresco website
| Search Immortality Topics: |
Category Archives: Neurology
Liraglutide (Victoza) superior to sitagliptin (Januvia) for reduction of HbA1c in diabetics
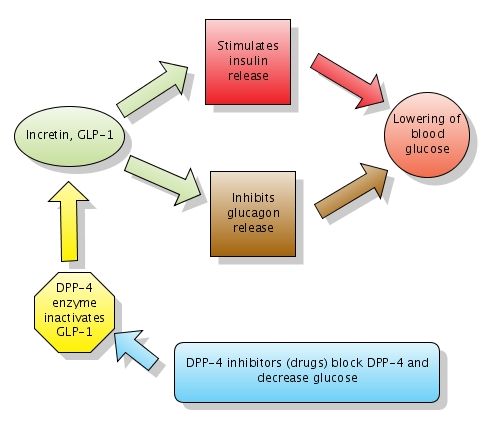
Action of DPP-4 inhibitors. Note that DPP-4 normally inactivates GLP-1. DPP-4 inhibitors block DPP-4 which in turn leaves GLP-1 active. Click to enlarge the figure. Created with Gliffy.
What is Glucagon-like peptide-1 (GLP-1)?
Glucagon-like peptide-1 (GLP-1) is a GI peptide that stimulates insulin secretion (similar to sulfonylureas). GLP-1 also inhibits glucagon release, gastric emptying and food absorption. GLP-1 and another similar peptide are called incretins. As noted above, incretins have a dual action which leads to lowering blood glucose:
1. Stimulate insulin release
2. Inhibit glucagon release
Exenatide (Byetta) is a GLP-1 receptor agonist approved for adjunctive therapy for patients with DM 2 who are not well controlled on oral agents. It is available only as injections and has to be administered twice daily.
DPP-4 inhibitors, or gliptins, increase GLP-1 levels by blocking the enzyme which inactivates GLP-1. The enzyme is called DPP-4 (dipeptidyl peptidase-4). They act similarly to Byetta (see figure above) but have the big advantage to be available in oral form (pills). Gliptins used for treatment of DM2 include sitagliptin (Januvia) and vildagliptin (Galvus).
What is Liraglutide?
Liraglutide (Victoza) is a long-acting glucagon-like peptide-1 (GLP-1) analog that was developed by Novo Nordisk for the treatment of type 2 diabetes. Liraglutide has a half-life after subcutaneous injection of 11–15 hours, making it suitable for once-daily dosing (in contrast to Byetta's twice daily).

Liraglutide. Image source: Wikipedia, public domain.
Liraglutide (Victoza) superior to sitagliptin (Januvia) for reduction of HbA1c in diabetics
This Lancet study assessed the efficacy and safety of the human GLP-1 analogue liraglutide versus the DPP-4 inhibitor sitagliptin, as adjunct treatments to metformin, in individuals with type 2 diabetes who did not achieve adequate glycaemic control with metformin alone.
More than 600 participants (aged 18—80 years) with type 2 diabetes mellitus who had inadequate glycaemic control (glycosylated haemoglobin [HbA1c] 7·5—10·0%) on metformin (more than 1500 mg daily) were enrolled.
Participants were randomly allocated to receive 26 weeks' treatment with 1·2 mg or 1·8 mg subcutaneous liraglutide once daily, or 100 mg oral sitagliptin once daily.
Greater lowering of mean HbA1c (8·5% at baseline) was achieved with 1·8 mg liraglutide (?1·50%) and 1·2 mg liraglutide (?1·24%) than with sitagliptin (?0·90%).
Nausea was more common with liraglutide (27%) on 1·8 mg. Minor hypoglycaemia was recorded in about 5% of participants in each treatment group.
Liraglutide was superior to sitagliptin for reduction of HbA1c, and was well tolerated with minimum risk of hypoglycaemia. These findings support the use of liraglutide as an effective GLP-1 agent to add to metformin.
References:
Liraglutide versus sitagliptin for patients with type 2 diabetes who did not have adequate glycaemic control with metformin: a 26-week, randomised, parallel-group, open-label trial. The Lancet, Volume 375, Issue 9724, Pages 1447 - 1456, 24 April 2010.
Posted at Clinical Cases and Images. Stay updated and subscribe, follow us on Twitter and connect on Facebook.
Posted in Neurology
Comments Off on Liraglutide (Victoza) superior to sitagliptin (Januvia) for reduction of HbA1c in diabetics
What’s new in nephrology and hypertension
 35% of UpToDate topics are updated every four months. The editors select a small number of the most important updates and share them via "What's new" page. I selected the brief excerpts below from What's new in nephrology and hypertension:
35% of UpToDate topics are updated every four months. The editors select a small number of the most important updates and share them via "What's new" page. I selected the brief excerpts below from What's new in nephrology and hypertension:
Glomerulonephritis
In idiopathic membranous nephropathy, among patients with protein excretion less than 8 grams/day, treatment with an ACE inhibitor or ARB increased the probability of remission.
Hypertension
There was no difference in the rate of myocardial infarction, stroke or death from cardiovascular causes between the intensive versus standard hypertension therapy groups, nor in the all-cause mortality rate. ('ACCORD BP trial'). Intensive therapy included goal systolic blood pressure less than 120 mmHg, standard therapy included goal systolic blood pressure less than 140 mmHg.
Hyponatremia
Tolvaptan is a vasopressin receptor antagonists. The long-term administration of tolvaptan appears to be safe and effective among patients with chronic hyponatremia. Responses were similar in heart failure and SIADH, and more modest in cirrhosis.
Transplantation
An increased incidence of angioedema has been noted in patients administered angiotensin-converting enzyme (ACE) inhibitors plus either sirolimus or everolimus.
Autosomal dominant polycystic kidney disease (ADPKD)
Activation of the mammalian target of rapamycin (mTOR) protein may contribute to cyst growth in autosomal dominant polycystic kidney disease (ADPKD). The inhibition of mTOR with rapamycin preserved renal function and inhibits epithelial cell proliferation and fibrosis in a mouse model of ADPKD. In a human trial, cyst volume was stable on rapamycin.
The long-acting somatostatin octreotide decreased liver volume by 5% in patients with autosomal dominant polycystic liver disease.
References:
What's new in nephrology and hypertension. UpToDate.
Twitter comments:
@kidney_boy (Joel Topf): UpToDate seems to be misrepresenting the ADPKD mTOR data. See my interpretation here: More ADPKD and sirolimus data: More definitive; less encouraging
Posted at Clinical Cases and Images. Stay updated and subscribe, follow us on Twitter and connect on Facebook.
Posted in Neurology
Comments Off on What’s new in nephrology and hypertension
In-flight exercises
 Prolonged immobilization can cause circulatory stasis which is one of the predisposing factors for DVT described by Virchow in his famous triad: endothelial injury, stasis and hypercoagulability.
Prolonged immobilization can cause circulatory stasis which is one of the predisposing factors for DVT described by Virchow in his famous triad: endothelial injury, stasis and hypercoagulability.
In a trial of previously healthy patients who traveled at least 8 hours per flight (median duration 24 hours), duplex ultrasound showed an asymptomatic DVT in 10 % of participants. In other studies, the reported risk of symptomatic DVT after flights of more than 12 hours was 0.5%. According to a 2006 Lancet study, activation of coagulation occurs in some individuals after an 8-hour flight.
This Chicago Tribune article lists some useful in-flight exercises:
In-flight exercises for beginners
- Shoulder shrugs, shoulder rolls. Ten each.
- Short sets of bending and straightening the elbows and knees.
- Walk through the plane every two hours.
- March your knees up and down in your seat.
- Lift and lower your feet on tiptoes to work the calves.
Advanced In-flight exercises
- Neck stretches; hold on each side for 15 to 20 seconds.
- If you can find space (near an exit), work the core with yoga stretches. Pigeon pose — an intermediate move of folding one leg under the body while stretching the back leg out — is an in-flight favorite of hers.
- In your seat, lift your arms over your head, grip your hands together and lean from side to side for a few seconds on each side. Repeat.
- Walk the length of the plane every hour, incorporating deep lunges. Unless you want air marshals on your case, it might be wise to notify a flight attendant.
- Put a small flight pillow in small of back to keep posture upright.
References:
Midair exercise makes for happier landings. Chicago Tribune, 10/2010.
Posted at Clinical Cases and Images. Stay updated and subscribe, follow us on Twitter and connect on Facebook.
Posted in Neurology
Comments Off on In-flight exercises
What’s new in gastroenterology and hepatology from UpToDate

35% of UpToDate topics are updated every four months. The editors select a small number of the most important updates and share them via "What's new" page. I selected the brief excerpts below from What's new in gastroenterology and hepatology:
Hepatitis C virus (HCV) infection
Peginterferon alfa-2a was superior to peginterferon alfa-2b with regard to virologic response rates in patients with chronic hepatitis C virus infection, genotypes 1, 2, 3, or 4. Patients being treated for chronic hepatitis C virus infection should receive peginterferon alfa-2a rather than peginterferon alfa-2b.
72 weeks of therapy with peginterferon alfa-2a plus ribavirin in patients with HCV genotype 1 or 4 was not better than 48 weeks.
Chronic use of proton pump inhibitors (PPIs)
Chronic use of proton pump inhibitors (PPIs) may lead to an increased risk of fractures. FDA recommends that healthcare professionals who prescribe proton pump inhibitors should consider whether a lower dose or shorter duration of therapy would adequately treat the patient's condition.
Ulcerative colitis
Once daily dosing of delayed-release mesalamine (Asacol 400 mg tablets) 1.6 to 2.4 g/day was as effective as twice daily dosing for maintenance of clinical remission in patients with ulcerative colitis. Remission rates were 85% in both groups.
Crohn's disease
Capsule endoscopy was not a cost-effective third test for establishing the diagnosis of Crohn's disease after a negative ileocolonoscopy and either a CT enterography or small bowel follow-through x-ray.
Azathioprine in combination with infliximab or infliximab alone had a higher rate of glucocorticoid-free clinical remission than those treated with azathioprine alone. Combination therapy and infliximab monotherapy led to significantly more complete bowel healing than azathioprine alone.
Obscure gastrointestinal bleeding
Double balloon enteroscopy (DBE) detected bleeding sources in 78% of patients with obscure gastrointestinal bleeding. Small intestinal ulcers and erosions were the most common findings.
References:
What's new in gastroenterology and hepatology. UpToDate.
Posted at Clinical Cases and Images. Stay updated and subscribe, follow us on Twitter and connect on Facebook.
Posted in Neurology
Comments Off on What’s new in gastroenterology and hepatology from UpToDate
Happiest people were 22% less likely to develop heart disease
 From WebMD:
From WebMD:
Happiest people were 22% less likely to develop heart disease over the 10 years of follow-up than people who fell in the middle of the negative-positive emotion scale.
People with the most negative emotions had the highest risk for heart disease and people who scored highest for happiness had the lowest risk.
Possible explanations for how happiness may protect the heart:
- Healthier lifestyle: Happy people tend to sleep better, eat better, smoke less, and get more exercise.
- Physiological impact: Happiness may produce a host of positive chemical changes -- such a reduction in stress hormones.
- Genetic influences: It could be that people who are predisposed to happiness are also predisposed to have fewer heart attacks.
Devote 15-20 minutes a day to doing something enjoyable and relaxing.
Strategies that could help naturally negative people become happier:
- Express gratitude on a regular basis.
- Practice being optimistic.
- Engage in frequent acts of kindness.
- Visualize one's best self.
- Savor joyful events.
- Practice forgiveness.
Regular exercise, sexual activity and good sleep are associated with increased self-reported happiness.
References:
Study: Happiness Good for the Heart. WebMD.
Image source: OpenClipArt.org, public domain.
Posted at Clinical Cases and Images. Stay updated and subscribe, follow us on Twitter and connect on Facebook.
Posted in Neurology
Comments Off on Happiest people were 22% less likely to develop heart disease
"Talk to Frank" – British government website for drug abuse prevention and treatment
Talk to Frank" is a British government-funded website for drug abuse prevention and treatment tips for the general public available at http://www.talktofrank.com
"A to Z" list of substances explains appearance and use, effects, chances of getting hooked, health risks and the UK law. It also includes information on peer pressure, etc.

Posted at Clinical Cases and Images. Stay updated and subscribe, follow us on Twitter and connect on Facebook.
Posted in Neurology
Comments Off on "Talk to Frank" – British government website for drug abuse prevention and treatment